Voted
Voted Empowering Survivors During Breast Cancer Awareness Month: Breast Reconstruction in Washington DC
Breast cancer is a life-altering journey that deeply impacts a woman’s physical and emotional well-being. For those who have undergone a mastectomy, double-mastectomy, or lumpectomy, the loss of one or both breasts can feel devastating. At Bruno|Brown Plastic Surgery, we are  dedicated to helping breast cancer survivors restore not only their physical appearance but also their confidence and sense of femininity. In honor of Breast Cancer Awareness Month this October, we want to highlight our comprehensive breast reconstruction services that empower women to reclaim their bodies and move forward with renewed self-assurance.
dedicated to helping breast cancer survivors restore not only their physical appearance but also their confidence and sense of femininity. In honor of Breast Cancer Awareness Month this October, we want to highlight our comprehensive breast reconstruction services that empower women to reclaim their bodies and move forward with renewed self-assurance.
Breast reconstruction can help survivors look and feel like themselves again by restoring or replacing the breasts after surgery. Every woman’s experience with breast cancer is unique, and so is her path to recovery. That’s why our plastic surgeons specialize in various breast reconstruction techniques, including tissue expander and implant reconstruction, DIEP flap (using abdominal skin and fat), pre-pectoral reconstruction, and more. During your consultation, we’ll work closely with you to evaluate your specific needs and goals, ensuring you receive the care and outcome that’s right for you.
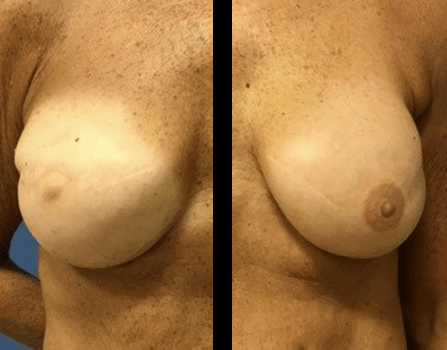
Welcome to our blog! If you’re looking for breast reconstruction before and after photos click here!
If you are interested in our breast cancer resources available click here!
A personalized approach to DC breast reconstruction
At Bruno|Brown Plastic Surgery, we believe that every woman deserves personalized care when it comes to breast reconstruction. Whether you’re looking for a natural reconstruction using your tissue or opting for implants, our experienced surgeons will guide you through the process, discussing options such as the DIEP flap, fat grafting, or breast implants. Our innovative techniques, such as muscle animation repair, help address any post-reconstruction concerns, ensuring that your results not only look good but feel natural and comfortable.
We understand that making decisions about breast reconstruction can be overwhelming, but you don’t have to face this journey alone. We encourage you to explore the resources we’ve gathered over the years, which our patients have found helpful. From breast cancer support groups to lymphatic massage services, these resources can help you navigate both your physical and emotional recovery. We are also proud to partner with Pink Perfect, offering custom-made nipples for those who want to add a finishing touch to their reconstruction.
Why choose Bruno|Brown for your breast reconstruction in DC?
Our breast surgeons in DC are leaders in breast reconstruction, with decades of experience and countless success stories. Our team is dedicated to helping each patient achieve the best possible outcome. We’ll review your options in detail during your consultation, ensuring that you feel confident and informed every step of the way.
To further support your recovery, we have created a comprehensive Breast Cancer Resources document on our website, offering additional tools and information to enhance your healing journey. You deserve the highest quality care as you take these brave steps toward reclaiming your life after breast cancer.
Schedule a consultation with our breast surgeon in Washington DC today and learn how breast reconstruction can help you feel whole again. Let us help you explore the possibilities and guide you through every phase of your journey.
Compassionate care for every step of your breast reconstruction journey
Breast reconstruction is about more than just restoring the physical appearance of your breasts—it’s about helping you regain your confidence and feel like yourself again. At Bruno|Brown Plastic Surgery, we are committed to providing compassionate, expert care to help you achieve your desired outcome. As Breast Cancer Awareness Month approaches, we invite you to take the first step toward healing by learning more about our services and scheduling a consultation. Together, we’ll work toward helping you feel beautiful, empowered, and whole again.